")


The cover story in the November issue of Christianity Today features two Harvard professors (Tyler J. VanderWeele and Brendan Case) who make a fascinating argument that empty pews in the aftermath of the pandemic may foreshadow a looming public health crisis.
A large share of Christians are opting to go it alone, moving their faith into quarters so private that even the church is not allowed in.
Obviously this trend drives down church attendance and membership. But less obvious until recently is that it is also harming the well-being of those who have stopped attending. A sizable body of research developed over the past couple of decades suggests that Glass’s story is a powerful instance of a broader reality: Religious participation strongly promotes health and wellness.
This means that Americans’ growing disaffection with organized religion isn’t just bad news for churches; it also represents a public health crisis, one that has been largely ignored but the effects of which are likely to increase in coming years.
The authors go on to summarize the research examining the public health benefits of church attendance.
So what are the public health benefits of church attendance? Consider how it appears to affect health care professionals. Some of my (Tyler’s) research examined their behaviors over the course of more than a decade and a half using data from the Nurses’ Health Study, which followed more than 70,000 participants.
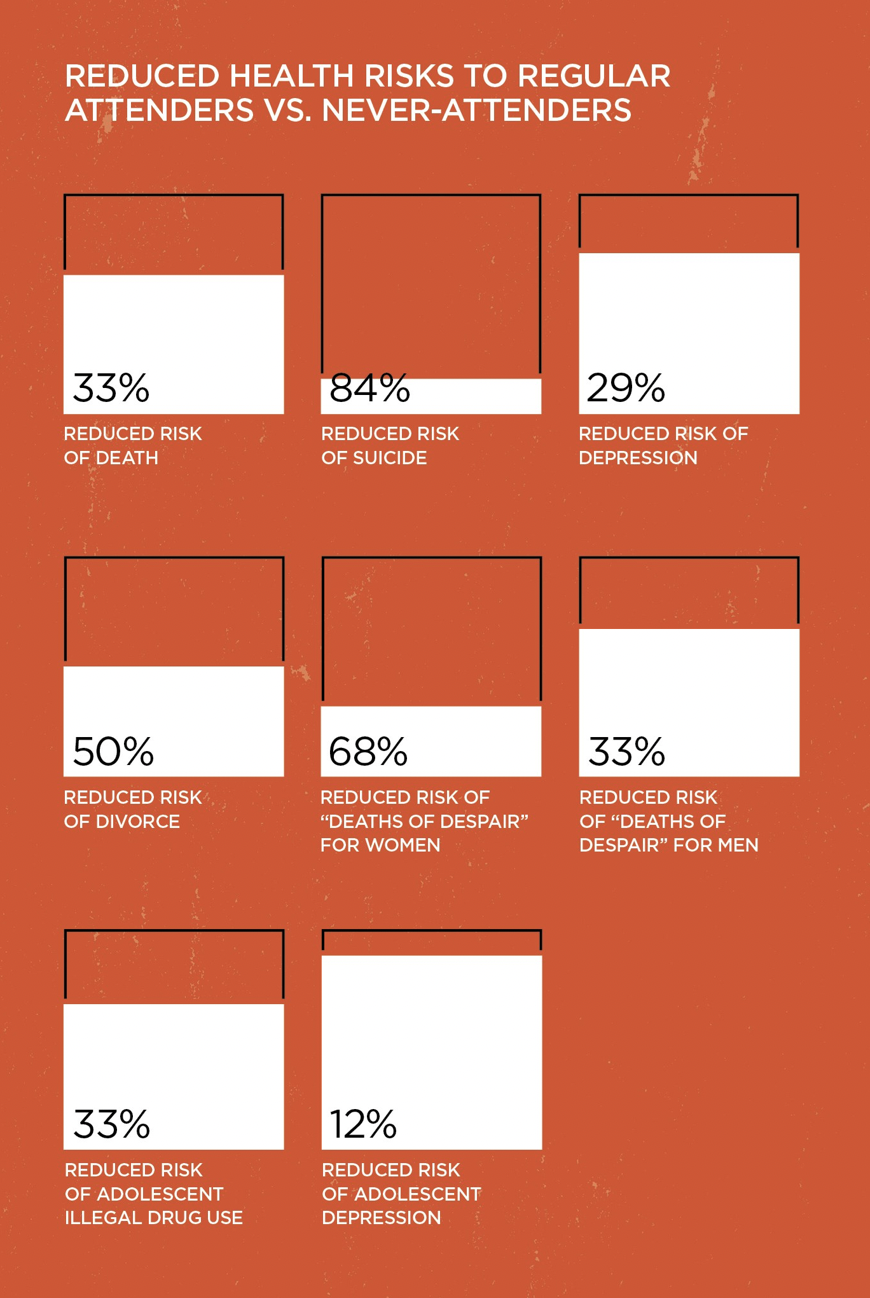
Medical workers who said they attended religious services frequently (given America’s religious composition, these were largely in Christian churches of one stripe or another) were 29 percent less likely to become depressed, about 50 percent less likely to divorce, and five times less likely to commit suicide than those who never attended.
And, in perhaps the most striking finding of all, health care professionals who attended services weekly were 33 percent less likely to die during a 16-year follow-up period than people who never attended. These effects are of a big enough magnitude to make a practical difference and not just a statistical difference.
From Christianity Today
A religious upbringing also profoundly affects lifelong health and well-being. We found regular service attendance helps shield children from the “big three” dangers of adolescence: depression, substance abuse, and premature sexual activity. People who attended church as children are also more likely to grow up happy, to be forgiving, to have a sense of mission and purpose, and to volunteer.
One of my (Tyler’s) most recent studies of health care professionals indicates that religious service attenders had far fewer “deaths of despair”—deaths by suicide, drug overdose, or alcohol—than people who never attended services, reducing those deaths by 68 percent for women and 33 percent for men in the study.
Our findings aren’t unique. A number of large, well-designed research studies have found that religious service attendance is associated with greater longevity, less depression, less suicide, less smoking, less substance abuse, better cancer and cardiovascular- disease survival, less divorce, greater social support, greater meaning in life, greater life satisfaction, more volunteering, and greater civic engagement.
As a Christian who spends a fair amount of time in an academic medicine environment growing increasingly hostile to anyone with traditional views of sexuality and gender expression, the presence of a large body of research supporting the public health benefits of church attendance and participation is very comforting. But what if the authors of these studies overlooked other possible explanations for the study findings that don’t show the church in such a favorable light?
One assumption in much of the research on the mental health benefits of church is that vulnerability to mental illness is equal among church attenders and non-attenders. What if that’s not the case? What if there’s something about church that leads to an overrepresentation of the “mentally healthy” compared to the general population? What if church is less accessible to individuals and families with a greater vulnerability to mental illness because the ability to engage in church activities self-selects individuals lacking the functional impairment seen in common mental health conditions. It was my observations that the families of kids served in my child and adolescent psychiatry practice were far less likely to be regular church attenders that provided the impetus for the establishment of Key Ministry.
Earlier this year, my daughter and I had a paper published in the Journal of Psychology and Christianity proposing a model for mental health inclusion in churches, grounded in the recognition of how functional limitations associated with mental health conditions often clash with “church culture”—defined as the expectations for how attendees will act and respond when gathered for worship, Christian education, missional service, social activities, and other functions of the local church. The qualities associated with mental illness negatively impacting church attendance include:
-
Stigma
-
Anxiety
-
Capacity for self-control
-
Sensory processing differences
-
Social communication
-
Social isolation
-
Negative experiences of church in the past
A more detailed description of the common barriers to church attendance and a model for implementing a mental health inclusion strategy is presented in Mental Health and the Church (Zondervan, 2018)
In fairness to Professor VanderWeele, he did control for differences in rates of depression in the study he conducted examining differences in suicide rates between health care professions who did and did not regularly attend religious services. In addition, the most compelling data demonstrating the impact of child and adolescent mental illness on family attendance at worship services wasn’t published until three years ago. The results of Andrew Whitehead’s study examining the relationship between disability and worship attendance are drawn from over 250,000 parent interviews conducted in three waves of the National Children’s Health Survey are presented below. I discussed the findings of the study here.
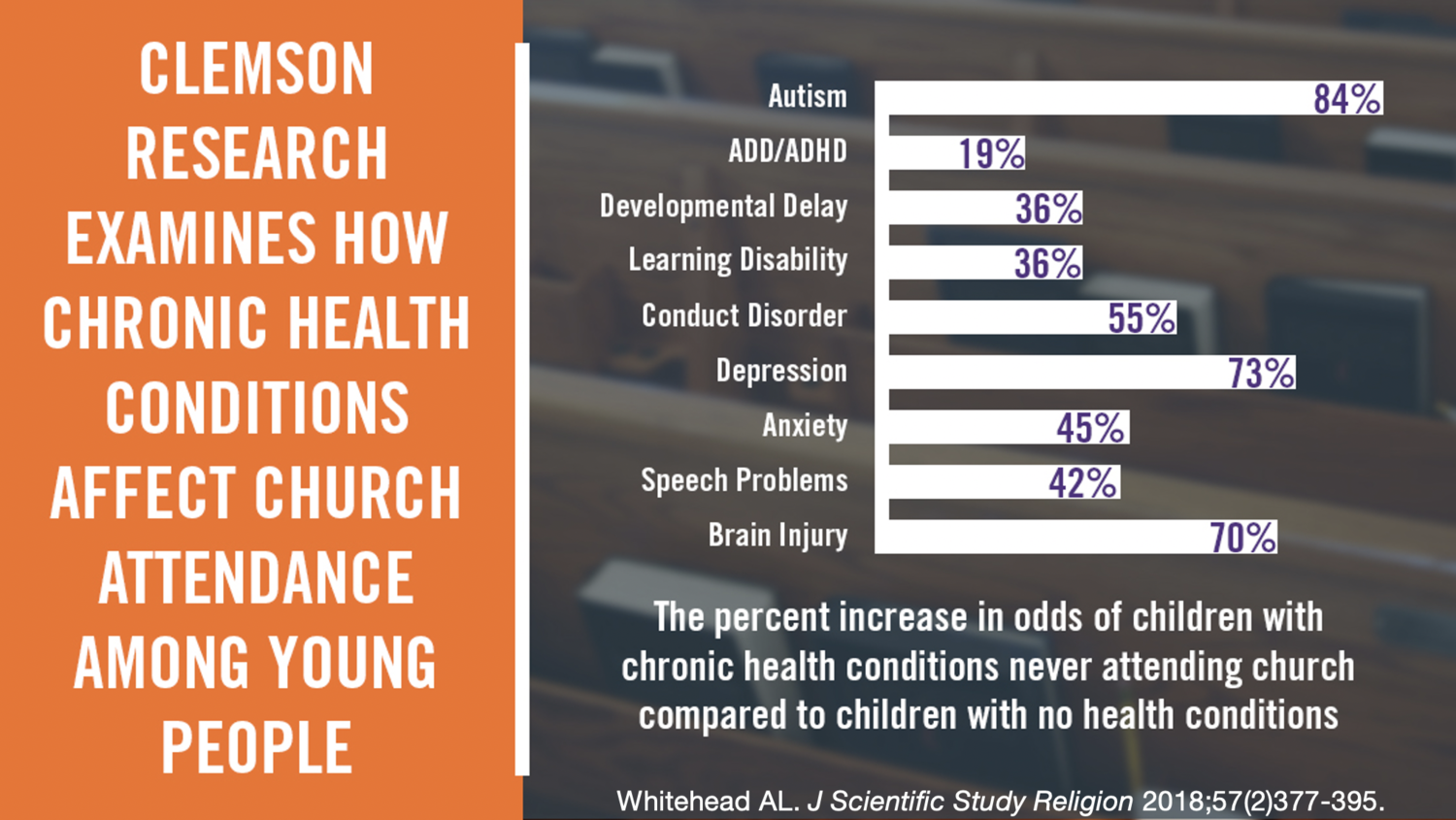
The percent increase in odds of children with chronic health conditions never attending church was 84.1% for children with autism spectrum disorders, 72.7% for children with depression, 54.6% for children with oppositional defiant disorder or conduct disorder, 44.7% for children with anxiety disorders, and 19.3% for children with attention- deficit/hyperactivity disorder (ADHD). Conditions not impacting church attendance included asthma, diabetes, Tourette Syndrome, epilepsy, hearing or vision problems, intellectual disabilities, and cerebral palsy.
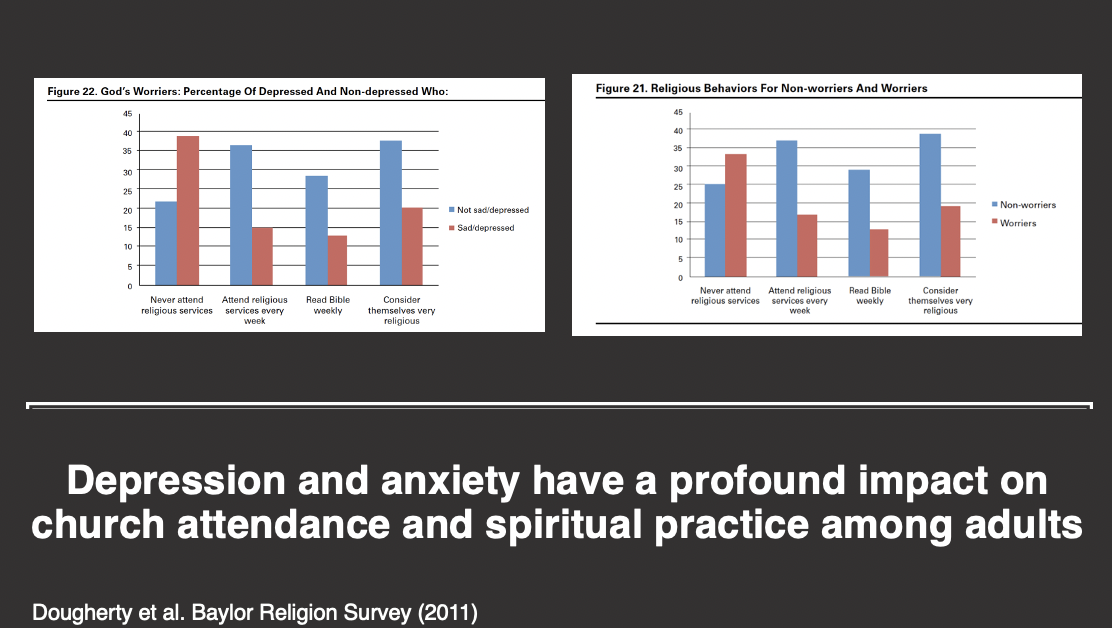
The data examining the relationship between church attendance and the presence of mental health conditions is less robust, but nevertheless worth consideration. In the Baylor Religion Survey, worriers—people who self-identified as feeling worried, tense, or anxious for ten days or more in the preceding month (17% of the U.S. population)—were less likely to have attended a religious service in the past year (67% vs. 75%), attend religious services on a weekly basis (17% vs. 37%), read the Bible on a weekly basis (13% vs. 29%), or consider themselves religious (19% vs. 39%) compared to non-worriers. Adults who experienced sadness or depression for ten or more days (11% of participants) during the preceding month were less likely to have attended a religious service in the past year (61% vs. 78%), attend services weekly (15% vs. 36%), read the Bible weekly (13% vs. 28%), describe themselves as “very religious” (20% vs. 37%) and more likely to identify as religiously non-affiliated (23% vs. 10%) compared to participants free of depressive symptoms.
Do our empty pews represent a looming public health crisis? We have a public mental health crisis NOW. Last week, the American Academy of Pediatrics, the American Academy of Child and Adolescent Psychiatry and the Children’s Hospital Association issued a joint statement declaring a national child and adolescent mental health emergency. Declining church attendance may reflect trends in the larger culture contributing to the rapid rise in mental illness.
Maybe a better way of thinking about the relationship between our rapidly expanding inventory of empty pews and the mental health of the population at large is to consider the obstacles that have made church attendance difficult for individuals and families struggling with mental health concerns is to consider how we as the church might build relationships with and serve the 20% of children and adults experiencing a mental health condition at any given time so that they’re drawn to sit beside us in the available pews at weekend worship?
Stephen Grcevich, MD is Associate Professor of Psychiatry at Northeast Ohio Medical University and President and Founder of Key Ministry.