


The featured article in this month's Journal of the American Academy of Child and Adolescent Psychiatry(JAACAP) is titled LGBT Youth, Mental Health, and Spiritual Care: Psychiatric Collaboration With Health Care Chaplains. As one of a very small number of Academy members in a position to comment on the cultural competency necessary in working with Christian families who adhere to traditional church teaching regarding sexual expression, I've been wrestling with how to best respond to the authors.
One reason this is such a big issue is that the authors are making statements in one of the most influential and prestigious journals in our field about what constitutes ethical care of youth with same-sex attraction not just for child and adolescent psychiatrists and other mental health professionals, but for chaplains providing spiritual care and support with children and teens in hospitals and other healthcare facilities.
After describing the two to fourfold greater risk of suicide among students who self-identify as members of a sexual minority, the authors make the following statement:
The religious/spiritual beliefs and traditions of LGBT youth, their families, and communities could be important related issues. Different religious and spiritual traditions hold various beliefs and attitudes about LGBT people, whose sexual orientation, gender expression, or identity might differ from family and social expectations and norms. Struggles over self-acceptance and whether to come out to others are typical, sometimes anguishing, challenges unique to these youths’ development. Health care chaplains might be uniquely positioned to help clinicians address mental health issues related to whether a patient’s spiritual/religious tradition is affirming or non-accepting of being LGBT—for culturally competent, humanistic care and to support positive clinical outcomes. This article discusses principles of health care chaplaincy for LGBT youth and families, opportunities for collaboration, and a framework for coordinating ethical chaplaincy and medical practice when religiously based stigma causes mental health risk.
In the paper, the authors present and discuss two case vignettes - one involved a college age student who had undergone male to female hormonal transitioning and struggled with body image issues upon following hair loss as a side effect of treatment for leukemia. The other vignette described a 15 year-old Latino boy from a devoutly Catholic family who verbalized to his father that the cardiac arrest that led to his hospitalization was a warning sign from God to "stop liking boys" - an interpretation his father agreed with.
Before making specific suggestions or criticisms of the approach they took in each case, I thought it important to seek to understand the thoughts and assumptions guiding their treatment. From the paper's abstract:
Lesbian, gay, bisexual, and transgender (LGBT) youth have unique medical and mental health needs. Exposure to stigma such as family non-acceptance is associated with adverse mental health outcomes that are important sources of morbidity and mortality in this population. These include depression, anxiety, substance abuse, suicidality, and risk behaviors that mediate exposure to human immunodeficiency virus and sexually transmitted infections. Different religious and/or spiritual traditions hold various beliefs and attitudes about LGBT people. These can be a factor influencing a youth's risk of experiencing stigma. Other unique developmental challenges of LGBT youth, such as conflicts over identity integration and disclosure, also can be influenced by religious/spiritual factors. Health care chaplains could collaborate with clinicians to support mental health by helping LGBT youth and families integrate religious with other aspects of identity, decreasing religiously based stigma, and supporting family connectedness.
This statement from the discussion section of the paper jumped off the page at me.
To serve widely diverse patient populations, chaplains take a nonjudgmental approach to the content of individuals’ beliefs and practices. However, chaplains can encounter stigmatizing attitudes among patients, families, or health care systems that increase risk for morbidity and mortality in LGBT youth. In providing spiritual care, chaplains can empathize with family concerns without validating stigma and preserve paths to novel solutions. They might discuss the meaning of LGBT identities or fears of non-acceptance in the context of a given faith tradition and explore awareness of accepting traditions. Chaplains can collaborate with psychiatrists to ensure that parents with non-accepting attitudes are aware of their risks and appropriate resources and help these parents process their religious commitments in light of evidence-based clinical recommendations. (Emphasis mine.)
To summarize the thinking of the paper's authors...
Stigma related to family non-acceptance of a student's sexual minority status increases risk of suicide.
Youth from spiritual traditions that are non-affirming of sexual contact between members of the same sex are at a higher risk of religiously-based stigma and hence, suicide.
Ethical approaches to reducing suicide risk in sexual minority youth might include directing the youth to places of worship within their family's broad spiritual tradition that affirm sexual expression in the context of same-sex relationships or encouraging families to "process their religious commitments in light of evidence-based clinical recommendations."
If the flagship journal of the child psychiatry academy is suggesting that clinicians and chaplains act ethically by urging youth with same-sex attraction to explore more "affirming" houses of worship than those in which they have been raised and families to "process religious commitments in light of evidence-based clinical recommendations," is there evidence to support their assumption that teens from "non-affirming" families and churches at greater risk of suicide? Let's look at the data.
It's generally accepted that suicide rates among kids from families with higher levels of religious commitment and worship attendance (predominantly Christian churches in studies conducted in the U.S.) are lowerthan those of kids from less religious families. In a three-generation study from Columbia University of families at high risk of mood disorders, parent belief in the high importance of religion was associated with an approximately 80% decrease in risk in suicidal ideation/attempts in their offspring compared with parents who reported religion as unimportant. The association of parental belief was independent of the offspring’s own belief in the importance of religion and other parental risk factors and was statistically significant. 85% of subjects in this study identified as Christian (59% Roman Catholic, 26% Protestant), and the mean age of subjects was 12.5 years.
Results of this longitudinal study of 9412 respondents from four waves of National Longitudinal Study of Adolescent Health indicate that religious activity participation is associated with reduced suicidal behaviors among adolescents but this effect declines as they approach adulthood. In adjusted models, weekly church attendance at baseline was associated with a 42% reduction in suicide ideation by Wave III. This study by the same author suggests protective effects of religiosity in reducing suicidal behavior were prominent in adolescence but not in young adulthood. Analysis showed the early adolescent period represented an important window of opportunity for preventing escalation of suicidal thinking and behavior. Another study of suicidality among predominantly Roman Catholic youth in Mexico demonstrated internal religiosity (personal convictions and beliefs) did not appear to protect against suicidal ideation, but external religiosity (frequency of church attendance) did exert a significant protective influence.
In all of these studies, religiosity had a greater impact upon suicidal behavior in female adolescents, and in no study was data broken out by sexual orientation.
The authors cited this article from 2011 in Pediatrics on the relationship between social environment and suicide attempts among self-identified LGB youth. In this study of over 31,000 eleventh grade students in Oregon, the 4.4% who self-identified as lesbian, gay, or bisexual youth were significantly more likely to attempt suicide in the previous 12 months, compared with heterosexuals (21.5% vs 4.2%). The risk of attempting suicide was 20% greater in "unsupportive" environments compared to supportive environments. A more supportive social environment was significantly associated with fewer suicide attempts, controlling for sociodemographic variables and multiple risk factors for suicide attempts, including depressive symptoms, binge drinking, peer victimization, and physical abuse by an adult. A problem with this study is there is no direct evidence that suicidal behavior was correlated with internalized religiosity, church attendance or involvement with religious traditions that prohibit same-sex sexual relations. The authors used the following assumptions to develop a composite index of the "supportiveness" LGBT students were likely to experience across 34 different counties in Oregon. Supportive counties were defined by:
The proportion of same-sex couples
The proportion of registered Democrats
The presence of gay-straight alliances in schools
School policies (nondiscrimination and anti-bullying) specifically protecting lesbian, gay, and bisexual students.
This study from Archives of Suicide Research examined the relationship between religious conflict, sexual identity, and suicidal behaviors among a self-selected sample of LGBT young adults (ages 18-24) who completed an online survey nearly twenty years ago. Subjects with parents holding anti-homosexual religious beliefs experienced a 1.565 x greater risk of suicidal thoughts in the last month and were more than twice as likely report a suicide attempt in the last year compared to other participants. The same study revealed leaving one’s religion of origindue to religious conflict was associated with a 1.335x greater risk of suicidal thoughts and a two-fold greater risk of a suicide attempt in the past year.
Another study drawing from a University of Texas research database of over 21,000 18-30 year-old students demonstrated that increased importance of religion was associated with higher odds of recent suicide ideation for both gay/lesbian and questioning students. For bisexual students, the importance of religion was not associated with suicidal behavior, while religiosity was protective against thoughts of suicide and suicidal attempts among heterosexuals. Lesbians and gays who reported that religion was important to them were 38 percent more likely to have had recent suicidal thoughts (52% more likely among lesbians). The study was limited by a lack of detail about whether a participant’s specific religion had stigmatizing views of sexual minorities.
In summary, here's what the available research suggests:
Religiosity appears to play an important protective role in protecting against suicidal behavior in adolescents. The protective effects of church attendance and religiosity appear to have a greater impact upon females than males, and may diminish during the transition to adulthood.
There is no data I could identify demonstrating increased risk of suicidal thinking or behavior in kids under the age of 18 resulting from parents or churches prohibiting homosexual contact.
There is data in studies of young adults with same-sex attraction reporting higher rates of suicidal thoughts and attempts among participants for whom religion has greater importance and higher rates of suicidal behavior among those who leave the religion in which they were raised.
In the absence of any data supporting an association between traditional religious beliefs and increases in suicidal thinking or behavior in children and adolescents, suggesting an ethical mandate exists to influence kids with same-sex attraction to leave their places of worship for more "affirming" congregations or suggesting parents need to "process their religious commitments in light of evidence-based recommendations" is extremely premature at best, demonstrates an extraordinary lack of cultural sensitivity and ignores the ways in which spiritual formation and church attendance may help mitigate the increased risk of suicidal behavior among sexual minority youth.
How might church attendance benefitsexual minority youth? What if the higher rates of suicide described in this population are related to earlier onset of sexual exploration?
We know family religiosity is negatively associated with lower rates of adolescent sexual activity, fewer sexual partners and delayed onset of sexual activity in teens. Here's a study suggesting the younger the age at which young men with same sex attraction begin to progress through developmental milestones of sexual identity - awareness, identification, sexual experience, and disclosure - the greater their difficulties with emotional dysregulation, sexual compulsivity, anxiety and depression in adulthood.
This study reported sexual minority youth, in comparison to heterosexual peers are twice as likely to have sexual intercourse prior to the age of 13, more likely to be sexually active and more likely to have had four or more sexual partners.
Let's look at some of the findings from this study out of the U.S. Centers for Disease Control on the relationship between sexual identity, sex of sexual contacts, and health-related behaviors among students in grades 9–12.
How is sexual orientation related to self-reported prevalence of "serious" suicidal ideation?
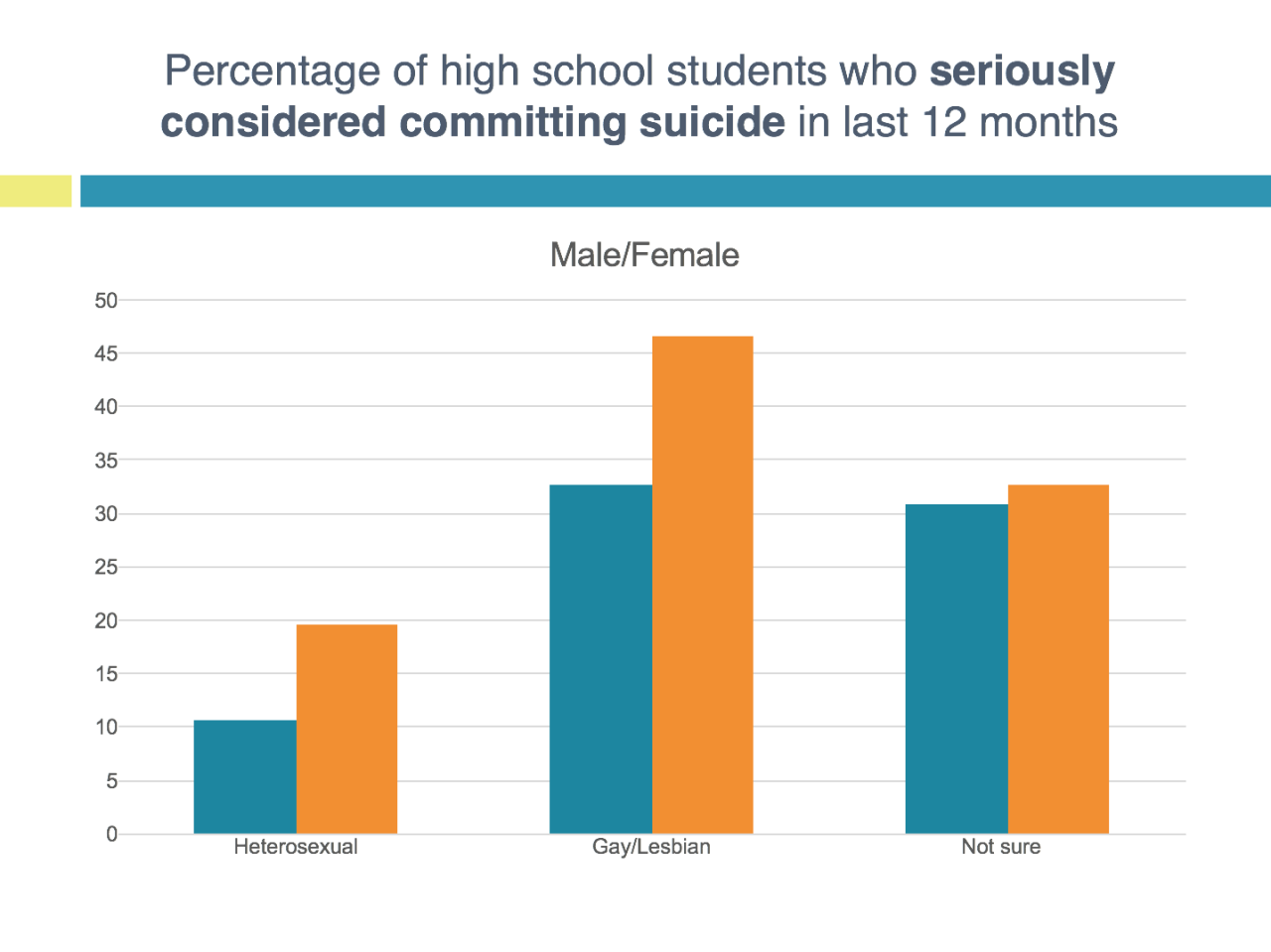
18% of U.S. high schoolers expressed "serious" suicidal thoughts in the past year - 15% among heterosexual students, 43% among LGB students, and 32% among youth identifying as "not sure" of their sexual orientation. Rates are clearly higher among females as opposed to males, consistent with what we know about sex ratios of suicidal ideation in teens. Two observations...
The frequency with which high schoolers across the board endorse the presence of serious suicidal thoughts is unacceptably high for kids of all sexual orientations.
The statistics describing rates of suicidal ideation among LGBQ teens are especially alarming and public health interventions targeted at reducing suicidal ideation and behavior among sexual minority youth are clearly indicated.
One approach the government has taken in response to the very high rates of reported suicidal ideation among sexual minority youth has been to implement anti-bullying strategies in schools across the country. The CDC made very specific support recommendations to schools for supporting youth from sexual minorities. LGBQ kids report more victimization from bullying than heterosexual peers.
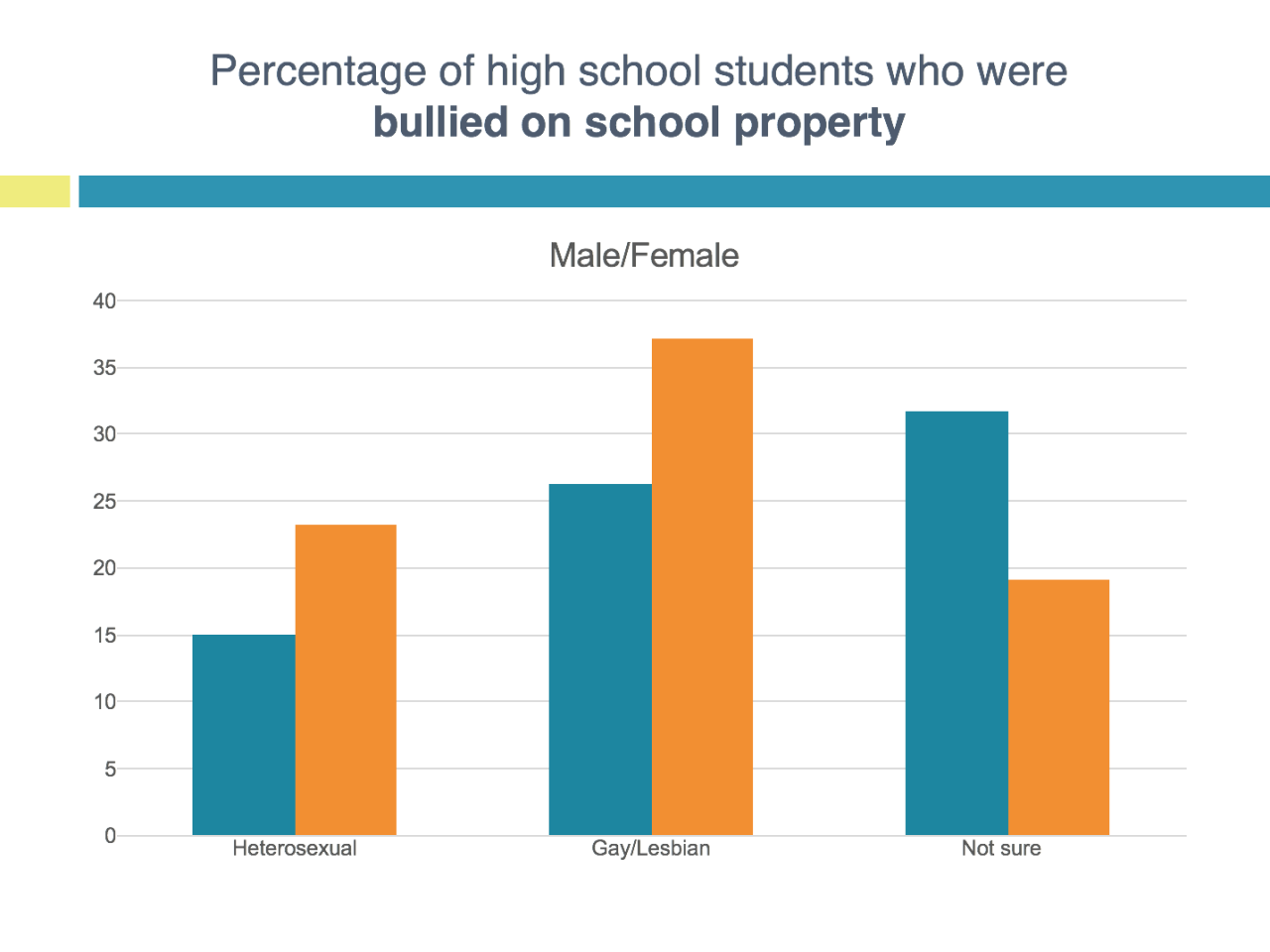
In the sample, 20.2% of all students; 18.8% of heterosexual students; 34.2% of LGB students; and 24.9% of "not sure" students had been bullied at school during the twelve months prior to the survey. Put differently, LGB students are about 80% more likely and "Q" students are about 30% more likely to be bullied compared to "straight" peers.
Let's examine the impact of sexual contact on suicidal ideation in teens.
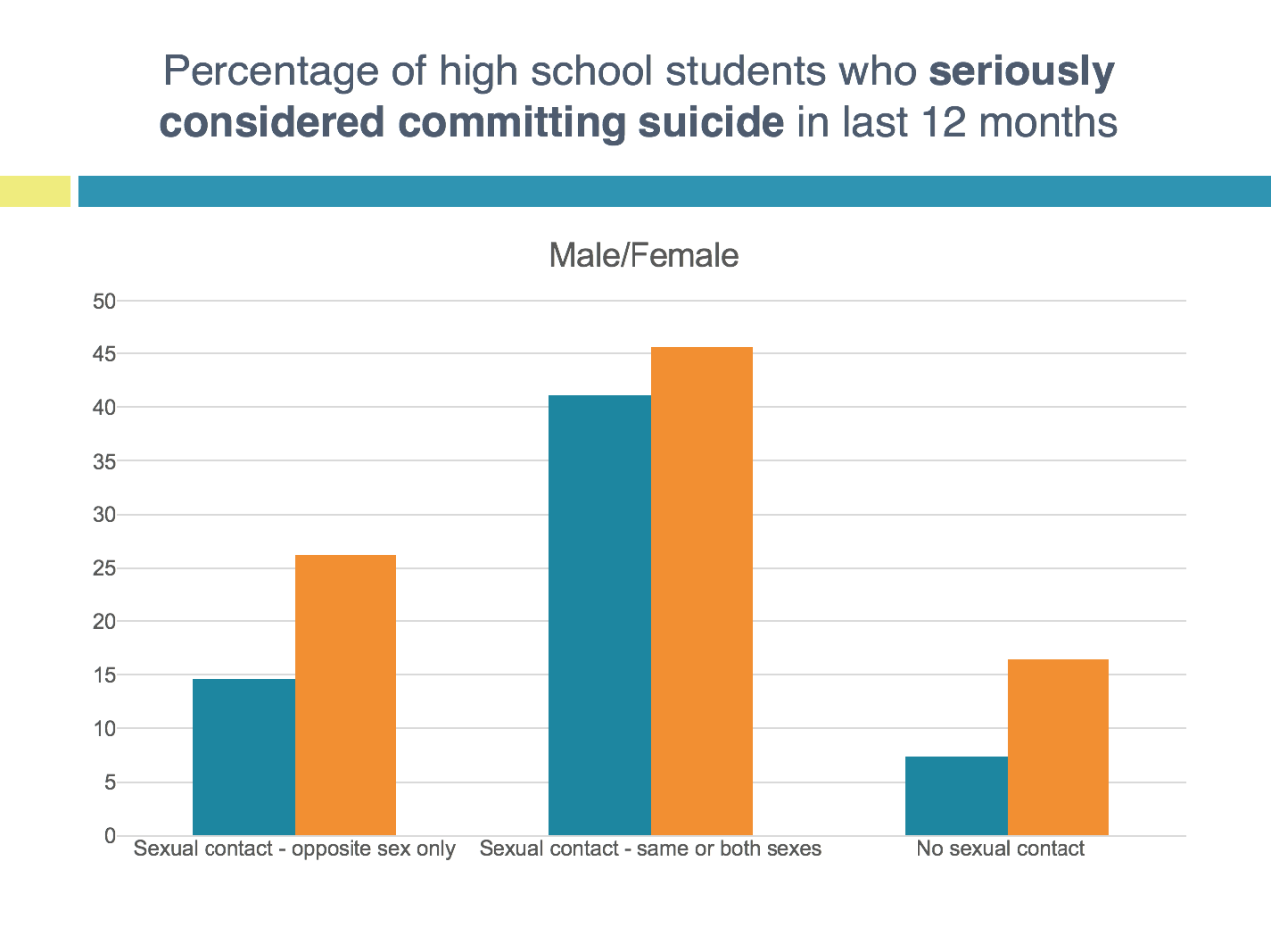
Overall, students who experienced sexual contact with the same or both sexes were approximately 225% more likely to experience serious suicidal thoughts than students who had sexual contact with the opposite sex only and 370% more likely to experience serious suicidal thoughts than students with no sexual contact.
Boys who experienced sexual contact with the opposite sex only were twice as likely to report serious suicidal ideation than those with no sexual contact.
Girls who experienced sexual contact with the opposite sex only were nearly 60% more likely to report serious suicidal ideation than those with no sexual contact.
Let's look at the data on high schoolers who developed a suicide plan...
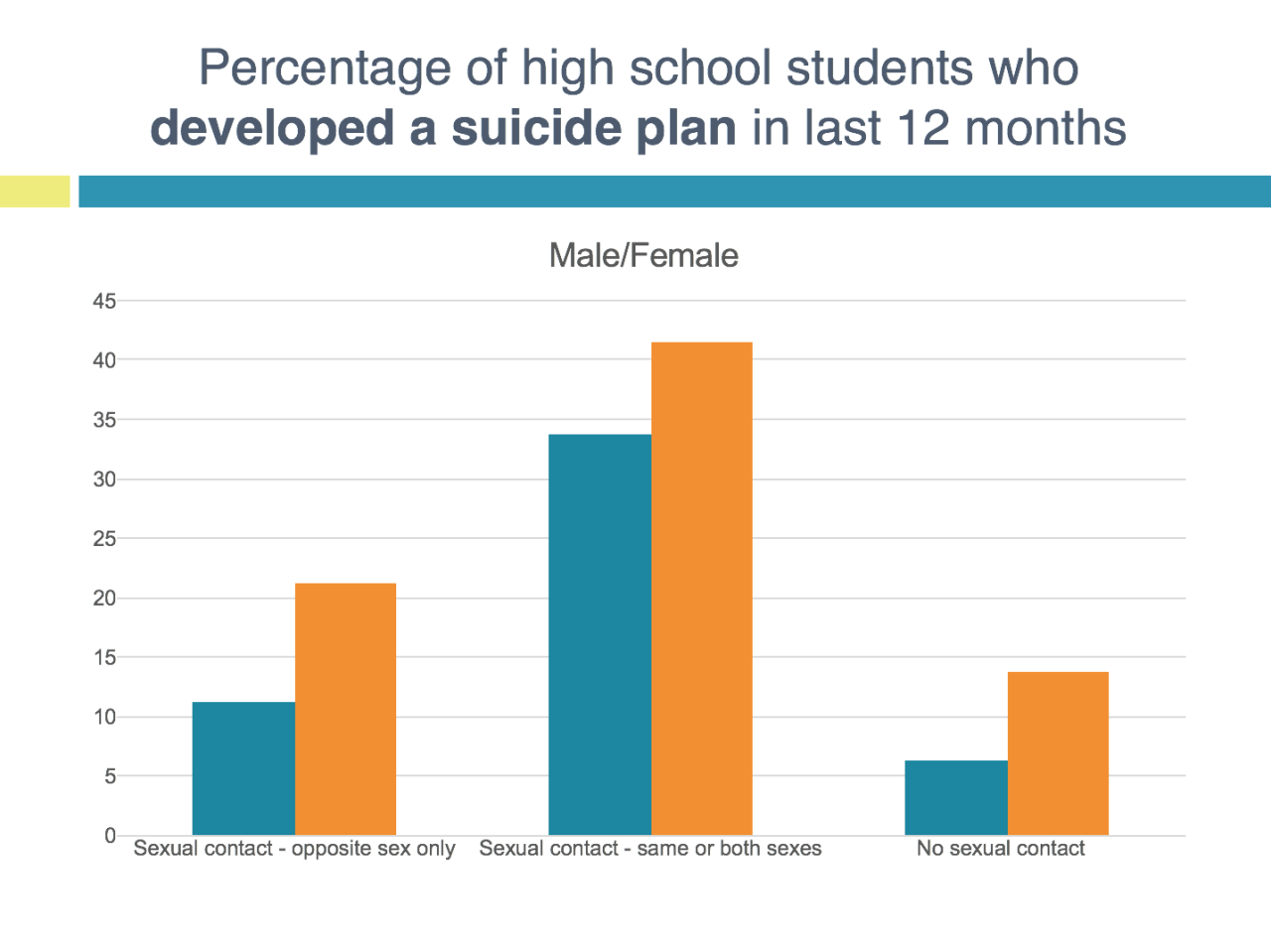
Overall, students who experienced sexual contact with the same or both sexes are approximately 250% more likely to report having developed a suicide plan than students who had sexual contact with the opposite sex only and 390% more likely to report having developed a suicide plan than students with no sexual contact.
Boys who experienced sexual contact with the opposite sex only were 78% more likely to report having developed a suicide plan than those with no sexual contact.
Girls who experienced sexual contact with the opposite sex only were 55% more likely to report serious suicidal ideation than those with no sexual contact.
Here's the data on suicide attempts and sexual contact...
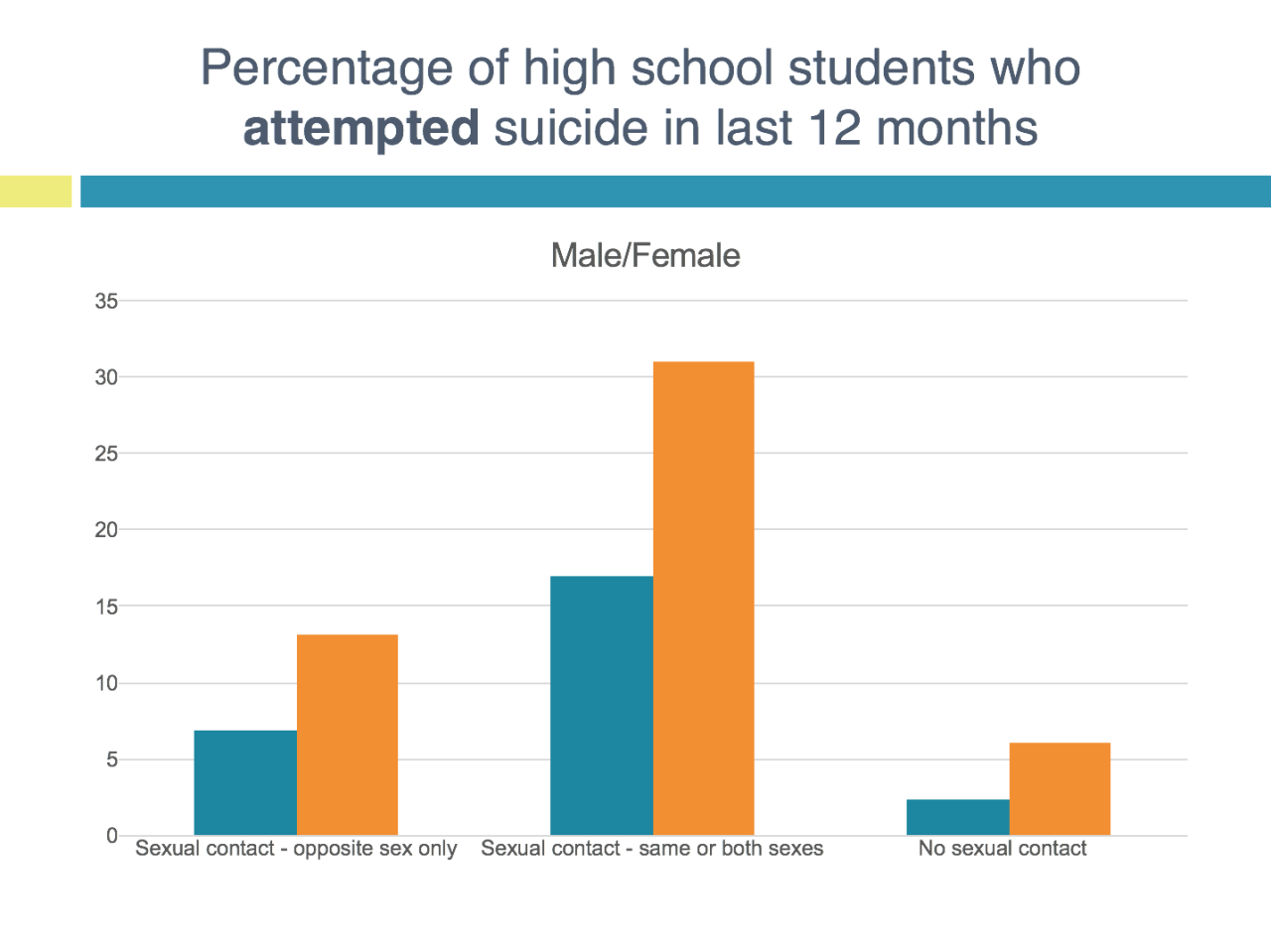
Overall, students who experienced sexual contact with the same or both sexes are approximately 285% more likely to report having attempted suicide compared to students who had sexual contact with the opposite sex only and 650% more likely to report having attempted suicide than students with no sexual contact.
Boys who experienced sexual contact with the opposite sex only were 215% more likely to report having attempted suicide compared to those with no sexual contact.
Girls who experienced sexual contact with the opposite sex only were 300% more likely to report having attempted suicide than those with no sexual contact.
Next, let's look at kids who received medical intervention as a result of a suicide attempt...
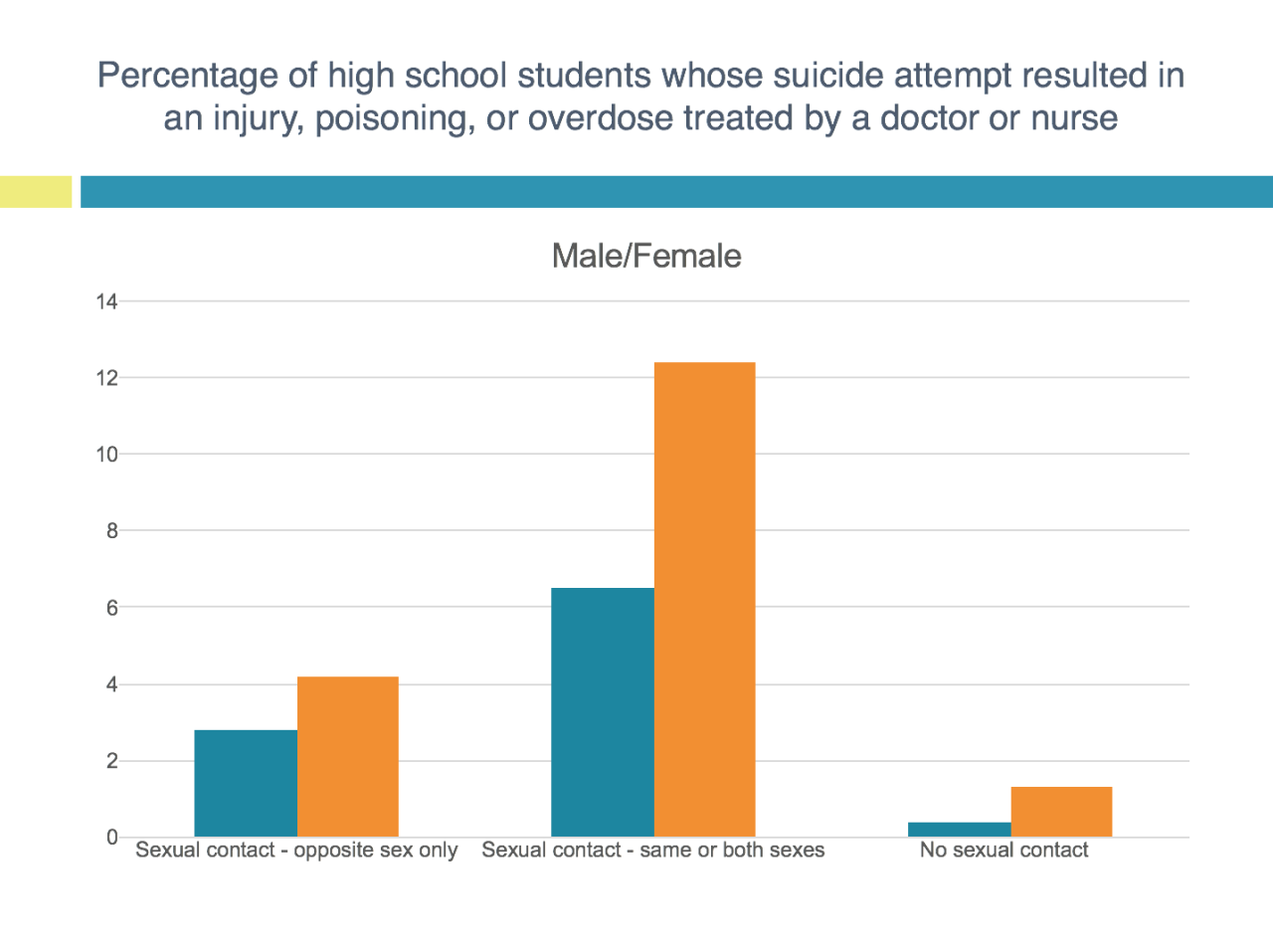
Overall, students who experienced sexual contact with the same or both sexes are approximately over three times more likely to have been seen by a doctor or nurse following a suicide attempt compared to students who had sexual contact with the opposite sex only and over twelve times more likely to have been seen by a doctor or nurse following a suicide attempt than students with no sexual contact.
Boys who experienced sexual contact with the opposite sex only were seven times more likely to have been seen by a doctor or nurse following a suicide attempt compared to those with no sexual contact.
Girls who experienced sexual contact with the opposite sex only were over three times more likely to have been seen by a doctor or nurse following a suicide attempt than those with no sexual contact.
The data suggesting a relationship between early onset of sexual behavior and suicide is overwhelming - yet we never hear about interventions to delay the onset of sexual activity as a strategy for reducing suicide rates in youth - especially sexual minority youth!
In conclusion... There is no clear evidence growing up in a family with traditional religious beliefs related to sexual expression or attending a church espousing traditional beliefs makes kids any more likely to attempt or commit suicide and overwhelming evidence that teens who delay the onset of sexual activity - gay as well as straight - are much less likely to struggle with suicidal thoughts or behavior.
Editor's note: One area in which I'm in agreement with the authors is in asserting there is no evidence that sexual orientation can be altered through therapy, and attempts to do so could be harmful
*************************************************************************************************************
Are you a pastor or ministry leader searching for resources to better understand how to support children, adults or families affected by mental illness in your church or in your community? Check out Key Ministry's Mental Health Resources page, containing links to video, articles and topical blog series designed to help you minister with persons with common mental health conditions. Also available through the website are a free, downloadable mental health ministry planning tool designed to accompany Mental Health and the Church, along with links to recommended books, like-minded mental health ministry organizations, relevant research, sermons addressing mental illness, social media resources and a compilation of stories from families affected by mental illness.

