

I was approached this past September by some folks with the Institute for Christian Anthropology about helping them develop resources for pastors, church leaders and Christian families addressing issues of identity, gender, and sexuality from a Judeo-Christian worldview. The resource they created—The Identity Project—has been launched and is now available online.
While gender identity has been at the forefront of our ongoing societal conversation in the last few years, why is this something an organization like ours would be asked to support? Why is it something I might talk about at a disability ministry conference?
We’re supporting this project because persons with disabilities are disproportionately represented among children and adults who embrace non-traditional gender identities. Leaders serving in disability or mental health ministry will greatly benefit from a deep understanding of gender and sexuality from a Biblical perspective. I’m spending part this week in an online forum on gender ideology with a fellow child psychiatrist, in which I’ll be reviewing data on the intersection of gender identity, sexuality, autism, mental health and disability.
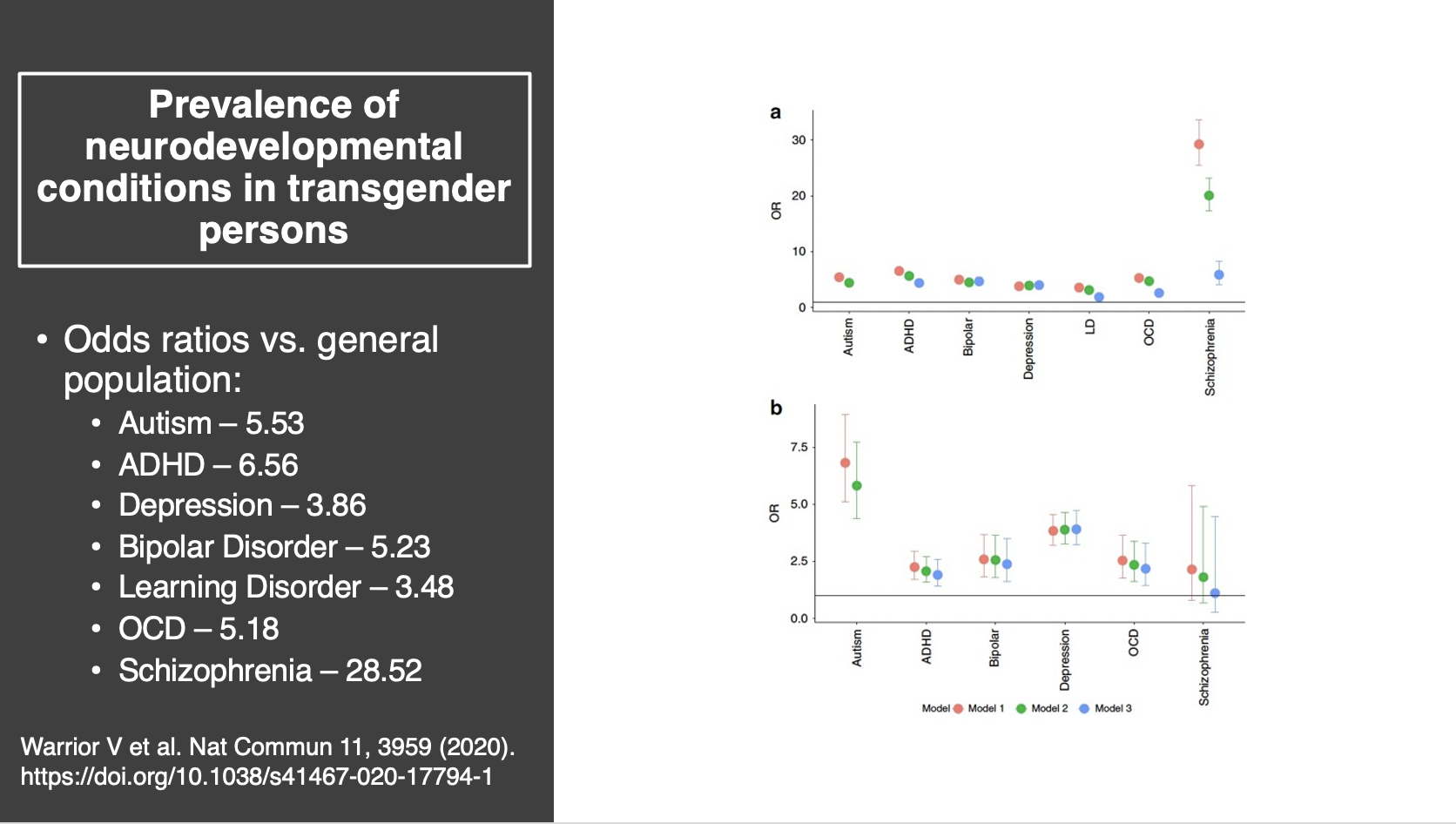
The data I’ll be reviewing, also shared below, is from the Human Rights Campaign, examining the prevalence of common disabilities in the LGBTQ community, as compared with the general population. Adults with transgender identity are more likely to experience every type of disability compared to the LGBQ population, with even larger differences reported versus the non-LGBTQ adult population.

Adults who identify as transgender are more than five times as likely to have received an autism diagnosis compared to the general population. They are six to seven times more likely to have received an ADHD diagnosis, more than five times as likely to have been diagnosed with bipolar disorder, experience elevated rates of learning disorders and OCD and are more than 28 times as likely to have been diagnosed with schizophrenia.
The severity and complexity of mental health concerns that characterize self-identified transgender adults is also seen in children and teens. This study examined rates of mental illness among 14–18-year-old students with transgender identity, obtained as part of a longitudinal study to evaluate the impacts of school-based mental health supports. A majority of transgender youth report clinical issues with anxiety or depression; more than half met criteria for non-suicidal self-injury and nearly half met screening criteria for post-traumatic stress disorder.
One of the speakers at our upcoming Disability and the Church conference became engaged in this topic after being contracted to create educational resources for families caring for children from the adoption and foster care systems, because the children in their care are disproportionately identifying as transgender. Trauma is consistently associated with gender dysphoria. An emerging body of research is demonstrating a connection between adverse childhood experiences, post-traumatic stress disorder and transgender identity.
This study looked at differences in mental health symptoms between transgender and LGBQ youth. Across the board, transgender youth reported more emotional abuse, physical neglect and emotional neglect compared to LGBQ youth. Adverse childhood experiences alone accounted for between 15-20 % of the difference in mental health outcomes between transgender and LGBQ youth.
From an evidence-based medicine perspective, many studies examining mental health outcomes in transgender youth are characterized by small sample sizes or short duration of follow-up. Large population studies from countries where all health information is collected in a single database are valuable, because they reduce biases introduced by the process through which subjects are selected for research studies. One such dataset available to researchers in the U.S. comes from the system that pays for healthcare for the military and their families.
This study reported mental health treatment information for all U.S. Military dependents with a diagnosis of gender dysphoria between 2010 and 2018. Youth who experienced “gender-affirming care” (defined as puberty blockers or cross-sex hormones) were compared to youth with gender dysphoria who didn’t receive puberty blockers or cross-sex hormones, as well as to siblings without gender dysphoria.
·Youth with transgender identity had a five-fold greater prevalence of mental health diagnoses compared to their peers.
·They used significantly more mental health services and psychiatric medication than their siblings.
The most fascinating finding is that trans youth receiving puberty blockers or hormones were receiving nearly 70% MORE psychiatric medication after initiating the gender-affirming care than they were before.
A topic of great interest among the families I serve is the connection between gender-affirming care and a diagnosis of autism in youth.
Until very recently, every family in the U.K. seeking gender-affirming care for their child was referred to the Tavistock Center, a clinic in London administered by the British Health Service. The clinic was shut down after an independent review commissioned by the British government led by Dr. Hillary Cass, a highly respected academic pediatrician currently retired from practice. One of the findings uncovered in the investigation was that 35% of patients who received puberty blockers and/or hormones through the clinic met criteria for moderate to severe autism. At the time of the investigation the reported prevalence of autism in the U.K was 2.1%. Kids on the autism spectrum were SEVENTEEN times more likely than their peers to receive medical treatment for gender transitioning.
This is a MAJOR concern to the families I serve in my practice. I’ve had parents of kids on the high end of the spectrum, or kids who are introverted or socially awkward, disclose they’re scared to death to take them to see a psychologist or counselor out of fear their child will be influenced to consider gender dysphoria as the cause of their emotional distress.
The most important point from these findings—at risk of being lost, as the care of the rapidly escalating population of kids with gender dysphoria has become politicized—is that kids wrestling with this stuff are extraordinarily fragile and vulnerable. They and their families desperately need our care and support.
I’d like to share some final thoughts with fellow Christians involved in ministry with kids and adults with gender dysphoria, because the research suggests you’re likely engaged in disability ministry.
Our churches need to be places where kids and teens wrestling with gender dysphoria and their families can experience belonging, even in situations when parents are following the recommendations of treating professionals and supporting their kids in social transitioning or use of puberty blockers and cross-sex hormones. From a Christian perspective, we can’t lose sight of the fact that their greatest need is Jesus. We know based upon research examining the relationship between childhood disability and family church attendance that families of kids with gender issues are far less likely to ever set foot in a church compared to friends and neighbors. One hypothesis for the spike in kids identifying as transgender is they’re finding belonging in online groups and forums that cater to that population. The kids—and their families—should be experiencing that sense of belonging at church.
Being kind to kids with gender dysphoria and their families is especially important. I can’t imagine anything more damaging to an adolescent’s spiritual development than experiencing cruelty or bullying from kids or adults they encounter at church.
We would want to avoid making kids with gender-related issues a focus of attention at church. What kids with mental health concerns and their families most want—and as we discussed earlier—most of these kids have SIGNIFICANT mental health concerns. What they most want, if they do come to church, is to blend in with everybody else. One obvious flashpoint is bathroom use. If your church facility doesn’t have a family restroom fully accessible for persons with disabilities, this might be a good time to build one.
Parents are an excellent resource and may have helpful insights for engaging and responding to kids when emotional, behavioral or gender-related issues arise at church.
Leaders within an individual church will want to consider how they might minister with persons with gender dysphoria and their families in ways consistent with their Biblical witness and identify “non-negotiables,” based upon their understanding of Scripture. For me personally, I’ll call kids by whatever name their parents want me to call them, since naming a child is a parent’s prerogative, but I won’t use pronouns inconsistent with biological reality. My job as a child psychiatrist includes promoting and reinforcing healthy reality testing among my patients. Supporting delusional thinking around gender that clashes with objective, biological realities is incompatible with healthy reality testing.


